

Download the audio
Watch on YouTube
The Pacific Islander Diabetes Prevention Program (PI-DPP), is a year-long, evidence-based lifestyle change program recognized and supported by the Center for Disease Control and Prevention (CDC). PI-DPP was formed through a partnership between the Association of Asian Pacific Community Health Organizations (AAPCHO) and the Pacific Islander Center for Primary Care Excellence (PI-CoPCE) as a project funded by the CDC DP17-1705 grant to scale the CDC National DPP in underserved areas. Currently, PI-DPP consists of 11 sites throughout the U.S. and U.S. Affiliated Pacific Islands (USAPI).
Aligning with DPP success standards, participants aim for 5% body weight loss, 150 weekly physical activity minutes (PAMs), and lower HbA1C values.
Listen in each week as we highlight PI-DPP sites. Mililani Leui, Program Manager of PI-DPP, chats with site representatives to hear about their community stories and program impacts.
This week we spoke with Romeo Alfred, Marcella Sakaio, Hemikko Bolkeim, Terry Lorok Jr., and Korab Lanwe of the organization, the Kwajalein Diak Coalition (KDC). KDC is located in Kwajalein, in the Republic of the Marshall Islands (RMI). In this episode, Mililani and the KDC team talk about the importance of tailoring the PI-DPP curriculum to their community’s needs as well as discuss their ongoing community projects focusing on healthy eating and diabetes prevention and management.
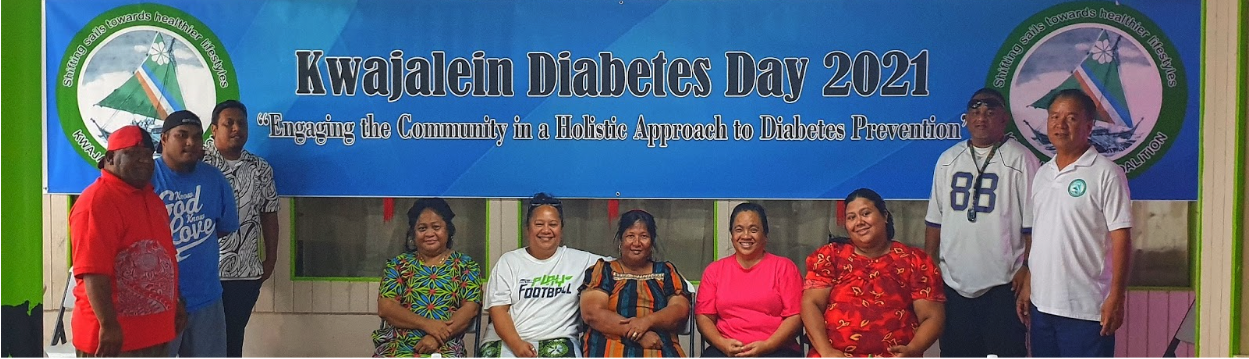
The KDC team pose for a photo on Kwajalein Diabetes Day 2021
Photo Courtesy of KDC
Marcella: This is Marcella Sakaio and I’m currently the hospital administrator here in Ebeye, and I’m also a lifestyle coach master [trainer] from Ebeye as well.
Romeo: My name is Romeo Alfred. I am the chairperson for the coalition, the Kwajalein Diak Coalition. My full-time job is an HR for the Telecommunication Authority in the Marshall Islands. As far as PI-DPP, I serve as a backup lifestyle coach.
Hemikko: Iakwe. My name is Hemikko Bolkeim. I’m the executive director for the Kwajalein Diak Coalition, and I’m also one of the lifestyle coaches for this year’s team.
Terry: Iakwe. My name is Terry Lorok Jr. And I’m the patient navigator for the coalition as well.
Korab: Hi, my name is Korab Lanwe. I’m actually the diabetes coordinator and also a lifestyle coach here in Ebeye.
Mililani: Thank you again for introducing yourselves. My name is Mililani, and I am the program manager for the Pacific Islander Diabetes Prevention Program.
So, the first question is, why is a program like this important for the community you serve?
Romeo: I think one of the primary reasons why this program is so important is because it’s one of a kind, there is no other program like it in the Marshall Islands. And also, just the fact that [from] the prevention aspect of things, this is really the only approach that we’ve seen so far that the government or the clinic in Ebeye is using [to] address the growing problem with diabetes in our community.
Marcella: And to add to that, as Romeo mentioned, prevention measures and healthy food selection, we know that the doctors have done a lot of effort in trying to tackle the diabetes issues here in Ebeye but have not really [been] successful on it. And with this kind of program, it got to continue what the doctors are or support what the doctors are doing at the clinic site, and since they’re all busy, we saw that we didn’t know how to come up with any program to help, especially the ones that are on the borderline for diabetes. We didn’t have any services or help for them. And this program really kind of answered our prayers where we wanted to prevent this diabetes since it’s a major issue, health issue, here in Ebeye.
This program really was the answer that we didn’t know that existed out there that fit our old way of living and put it back into practice again. The doctors can only do so much for the community members.

KDC Cooking Demonstration for Participants
Photo Courtesy of KDC
Mililani: Why is it important to tailor the program to your community’s specific needs?
Romeo: On the economic side, we do not have adequate resources to keep managing the disease after its onset. On the environmental side, we are a country that is vastly isolated from the rest of the world. So seeking medical attention outside of the Marshall Islands is not an option for a majority of our population.
And on the political side, for ages, we’ve heard our leaders publicly declare, our prevention is the only logical pathway to address the chronic nature of diabetes in our islands. Yet very little is done in the area of prevention, if any. Nothing has been done in that area. So no concentrated effort has ever been placed on prevention.
Marcella: And to add to that, it’s like [a] community helping community whereas when it goes into politics or the government, it goes somewhere else instead of the community that really have needs for these kinds of services or help.
Mililani: Is there any background information you would like to share to reinforce the importance of this program for your community?
Romeo: There’s just so many background information that we can share, but the ones that really stand out, if we go back to when we first started this organization, and we go back way before PI-DPP. There was a lot of stigma around the disease that we recognized. And so it was very difficult to come up with a strategy. We had sat down together so many times in trying to come up with a plan. It was quite difficult. But having collaborated with so many organizations outside of the Marshall Islands, regionally and internationally, it opened our eyes up to a lot of things, including providing us hope that some level of help is out there.
I can remember, specifically, the meeting, one of our strategic meeting(s) early on, somebody within the group came up with this idea that from the movie, Field of Dreams, the catchphrase from that movie, they say, “If we build it, they will come.” So that was essentially one of the catchphrases that provided [us] with the hope and the concept that if we build something and work out of it, then soon enough we will find people coming to us for help and as well as organizations coming to us for support.
And not only community members with the disease, but also people outside of the Marshall Islands, regionally and internationally, that can readily provide support.
Marcella: It was a matter of us bringing out the needs, the community needs. Locally we don’t have farming here in Ebeye, but we explore some ideas of importing from other places. There was really nothing to offer to assist people with high prices to get local food or healthy food.
It was through all these, I guess, experiences that we were able to bring other outside people to come and try to help us with, especially local farming food. So, currently we have the Taiwan farming happening in Ebeye. I know it has also, I guess, influenced our traditional leaders for trying to get back to our local food and program.
 |
 |
|---|
KDC 2017-2022 Impact Report
Photo Courtesy of PI-DPP
Mililani: What impact has your site had on the communities you serve?
Romeo: I can start with the impact that we have within the service provider itself, and I’m referring to the clinic, the hospital as an organization. One thing that was very obvious early on was the number of people that were coming to their weekly clinics. There was only a few back then. How do we get people to realize that these are clinics that the population, the community needs to better understand, not just how to properly manage the disease, but also strategies on how to prevent members of the community, in the first place, [from getting] to get diabetes.
If you compare that back then to now, the hallway is practically crowded every time you come in [during the weekly diabetes clinic in Ebeye]. Just seeing how the number of people have increased from back then, it gives us hope that something good is happening. The services that we’re providing to the community has an impact. A notable impact on the community.
Marcella: It has to do with educating people because [the] hospital is kinda like a scary place for everybody to come and check where you are. But somehow that was a thousand people feel comfortable coming to– a lot of our participants didn’t even know what their height was and their weight. It wasn’t important to them to know. Even if they’re not sick, they can just come and check what their A1Cs or want to know what their weight are.

Photo and Description Courtesy of KDC
Romeo: Later on, we have decided to set up a public garden at the hospital outside of the hospital. And we did that. We did that using the skills that we got from the classes that was done by one of our partners. And so, we built this garden at the hospital and when people started seeing that the garden was actually producing vegetables, and some of them came back and asked that we give them the seeds and pots that they had once refused to take because they weren’t comfortable that they would be successful. These days when you go to Gugeegue, a nearby community by the causeway on Ebeye, you see people actually growing vegetables. It is encouraging to see these kinds of developments among the community.
Hemikko: After taking the classes, they’re so excited that they plan to plant their own vegetables and after meals at home.
Romeo: I can now look back and see the first organization that we partnered with. They have this idea that they want to introduce an all-green recipes to the community. And then because we are from the community and we understand that, to a great extent, the diet the population prefers is meat based.
And so we knew already, because we’re a member of the community, we know already that this is not going to work. So instead of going straight to an all green diet, we introduced green to existing recipes that they were already using or ones that we introduced to them in our cooking demonstrations. We said, “Well, you know, let’s do this slowly. ” Even do palatability testing. So they’re the one(s) that select the type of recipes that they like. So it’s all based on their palatability.


Photos and Descriptions Courtesy of KDC
Mililani: What are some of your site’s challenges and/or best practices for recruitment, retention and general programming?
Romeo: When we first started to introduce home gardening, we brought in partners from outside (RMI) to help us entice people into setting up their own gardens. And one of the examples that stood out was we brought in gardening materials, and after we do classes, teaching them the proper way of doing home gardening. Even after the class, people still returned the supplies and materials that we distributed to them. And this was simply because the trials that they have done in the past weren’t that successful. And so they were thinking, “Oh, here’s another thing that they’re trying to teach us, but it will never work because of the condition of the soils and all the limited areas that we have within the community.” So all these gave a reason for members of the community to be discouraged. And so these are big challenges that we had to face when we started out this program as a group.
As we shared our experience with other partners and in the region, other groups that are also doing their own PI-DPP program in their islands —places like Kosrae, Chuuk. So we all recognize that we have some common challenges when we first introduced the PI-DPP program. It all boils around mostly retention. Early on when we did the screening and when we formed our classes together, we used to do a pre-select place that we do these programs and we [later] realized that we were losing attendees. When we look closer at why we were experiencing all these issues, we recognized that we weren’t really focusing on what the participants want, what they prefer [but rather wanted what was convenient for us]. And it was from all these sharing with other groups in different islands like, for example, Kosrae, Kosrae was doing theirs at their churches.
And so we picked up on that and said, “Let’s try the strategy that Kosrae is doing.” And we sat down and we realized that it was attracting more attendees and retention was a bit higher than when we were doing it in just a classroom that we had set up ourselves. And so we made these changes to address the challenges as we come across. Sharing our experiences with groups from neighboring islands helped.
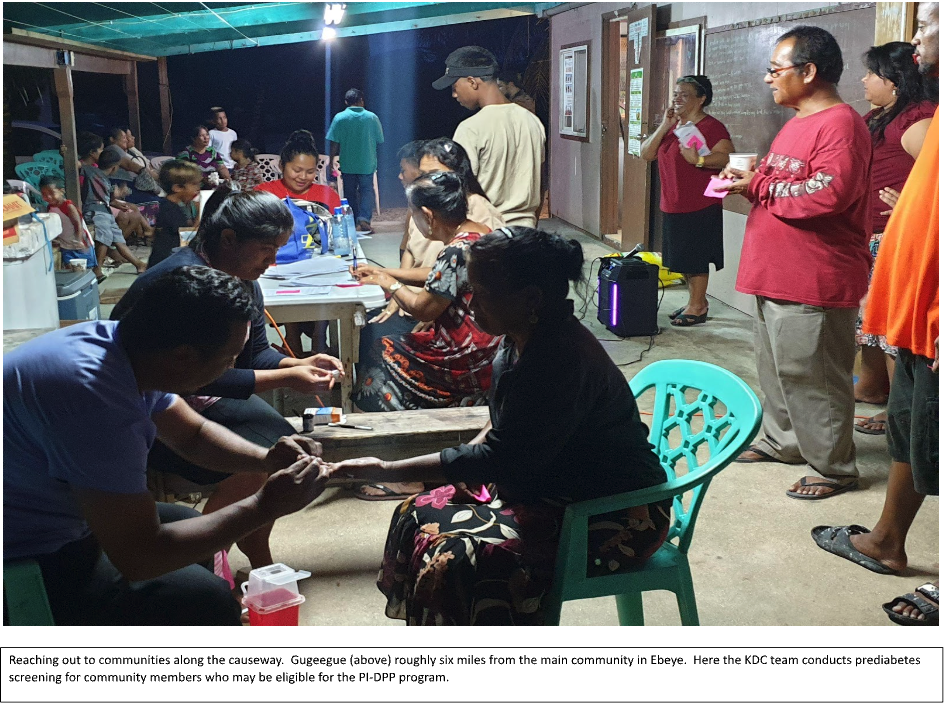
Photo and Description Courtesy of KDC
Marcella: I think the best we can say, we faced a lot of challenges in addition to what Romeo said when we started. And I guess I’d like to say we learn as we go or went because holding our classes to an assigned place wasn’t really working out well for us. So we started with the work site and these were also ideas from other sites. And for Ebeye alone, we also learned that when we go through the churches, it worked best for us. So that’s where instead of creating a classroom and calling everyone to come to it, a regular classroom setting, we went to where they were comfortable with. So that was their environment, church environment. In a way, I think looking at our participants’ wants and needs help(s) us with many of our challenges.
Romeo: Another aspect of what we picked up on was that all of us have full-time jobs. It’s quite challenging making the time and effort to apply to this program. But considering that we were able to develop this program and sustain it over a more than a ten-year-period, I think that’s something to be proud of.
Mililani: What future projects and or goals does your site have for advancing diabetes prevention and promoting healthy lifestyles?
Romeo: And one of the things that we’re seriously considering is institutionalizing these programs, so that they complement existing setup or programs within an organization. And for example, right now we focus a lot on including our program in church activities. And so we’ve been talking about now that Marcella is a master coach, maybe teaching lifestyle coaching in the churches. We can have a group of lifestyle coaches within each of the church denominations.
We feel that institutionalizing this program into existing programs within each of these organizations will help sustain this program over the long period.
And so, we do have existing setup with the government that have different focus. I guess using the data that we’ve collected over this five year period to use when we approach our government for either additional funding or just the existing funding that we’re receiving from them. But we focus it, so it can also include the PI-DPP program.
In terms of the way forward, we have a fully established relationship with the clinic here. The clinic focuses primarily on managing diabetes while KDC focuses on the prevention aspect of the disease. And so this is something that we had set up among ourself, us, and the clinicians here at the hospital. It’s something that both group supports and it will continue to be one of our strategy forward.
We thank Romeo, Marcella, Hemikko, Terry, and Korab from the Kwajalein Diak Coalition for speaking with us during this week’s segment. Please stay tuned for our next site highlight!
To learn more about KDC, please visit their website Facebook page at https://www.facebook.com/KwajDiakCoalition/.
To support KDC in their pursuit of diabetes prevention and promoting healthy lifestyles, please contact Hemikko Bolkeim at hemikko.bolkeim@gmail.com for more information.
Be sure to learn more about Romeo’s work and check out why he is an #AANHPIhealth Hero!
Facebook: @KwajDiakCoalition
Leave A Comment